Heath Dorion, MD, Brian Gruber, MD
Surgical-site infection requires microbial contamination of the surgical wound to occur. The microorganisms may originate from either endogenous or exogenous sources.
Sources of endogenous flora include the patient’s skin, mucous membranes, or hollow viscera. Exogenous flora originate from any contaminated items on the sterile surgical field including surgical team members, instruments, air, or materials.1
Infection only occurs if the number and virulence of the bacteria or fungi overwhelm natural host defense mechanisms. Typically >105 microorganisms per gram of tissue must be present for infection to develop, unless foreign material is present in the surgical site (ie, suture, mesh).1
RISK OF SSI
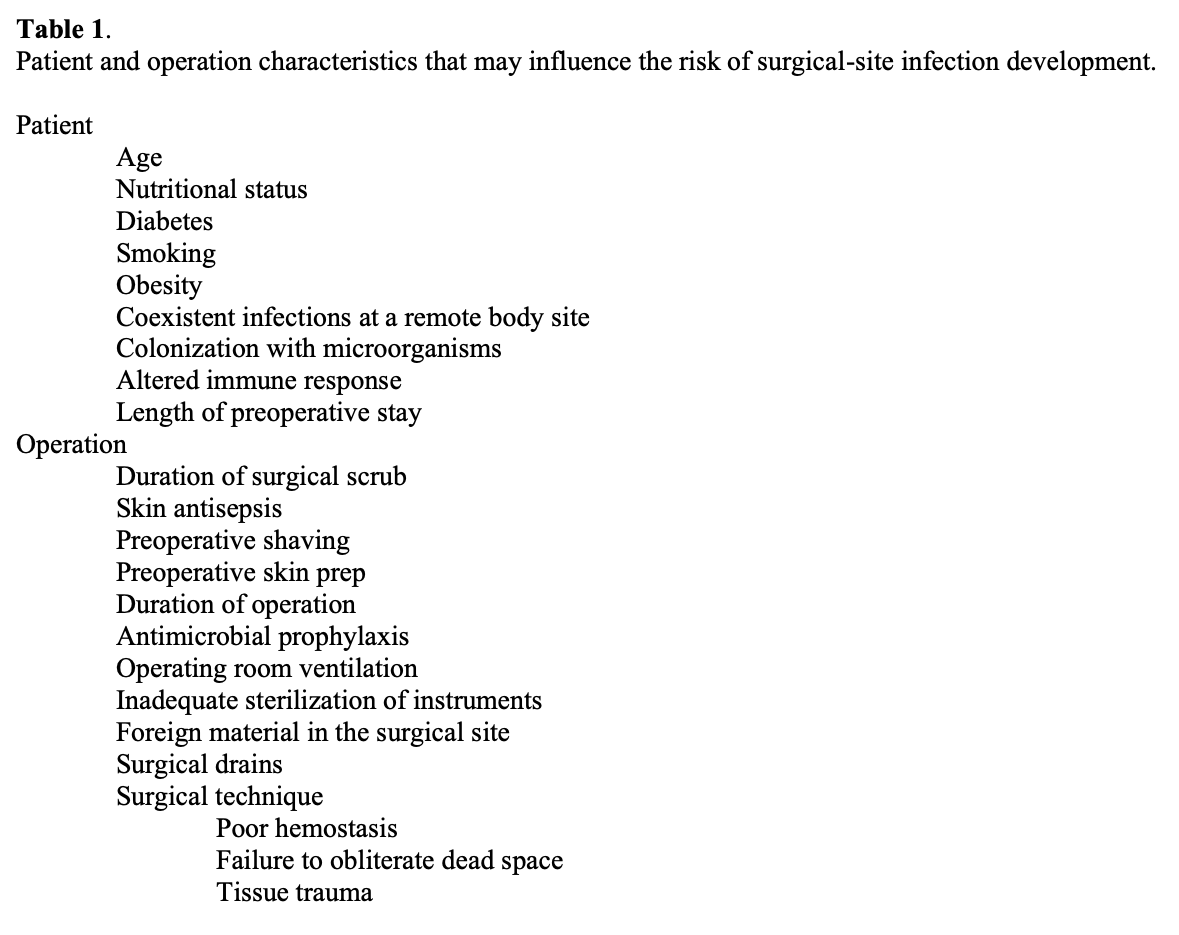
The Hospital Infection Control Practices Advisory Committee of the Centers for Disease Control and Prevention published guidelines for the prevention of surgical-site infections in 1999. Both patient and operation characteristics were examined to determine risk factors and prevention measures pertinent to surgical-site infection. The patient characteristics found to possibly increase the risk of SSI included diabetes, nicotine use, steroid use, malnutrition, prolonged preoperative hospital stay, preoperative nares colonization with Staphylococcus aureus, and perioperative transfusion. In addition, older age, obesity, remote body site infection, and systemic immunocompromise may increase risk of SSI (Table 1).1-3
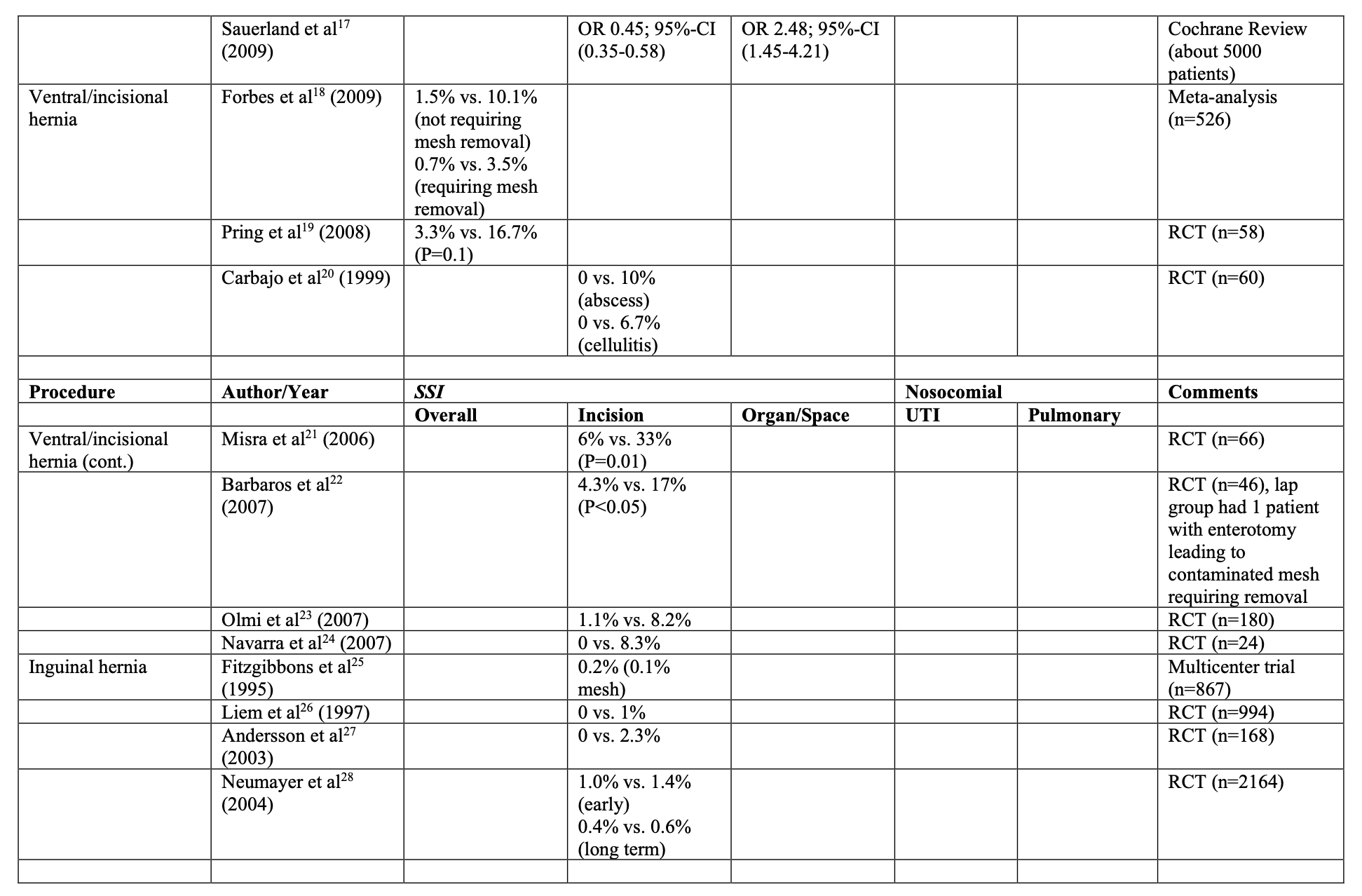
Utilizing laparoscopic instead of open techniques in surgery results in lower rates of SSI (Table 2).3-28 Diagnostic laparoscopy reduces the chance of an incisional SSI by 60% and organ/space SSI by 80% compared with open diagnostic exploration of the abdominal cavity.29 Smaller incisions in laparoscopic procedures reduce postoperative pain resulting in shorter hospital stays, quicker mobilization, better pulmonary toilet, and earlier bladder catheter removal. In addition, there is a decreased incidence of postoperative ileus and less need for central venous catheterization for administering parenteral nutrition.3,30-32
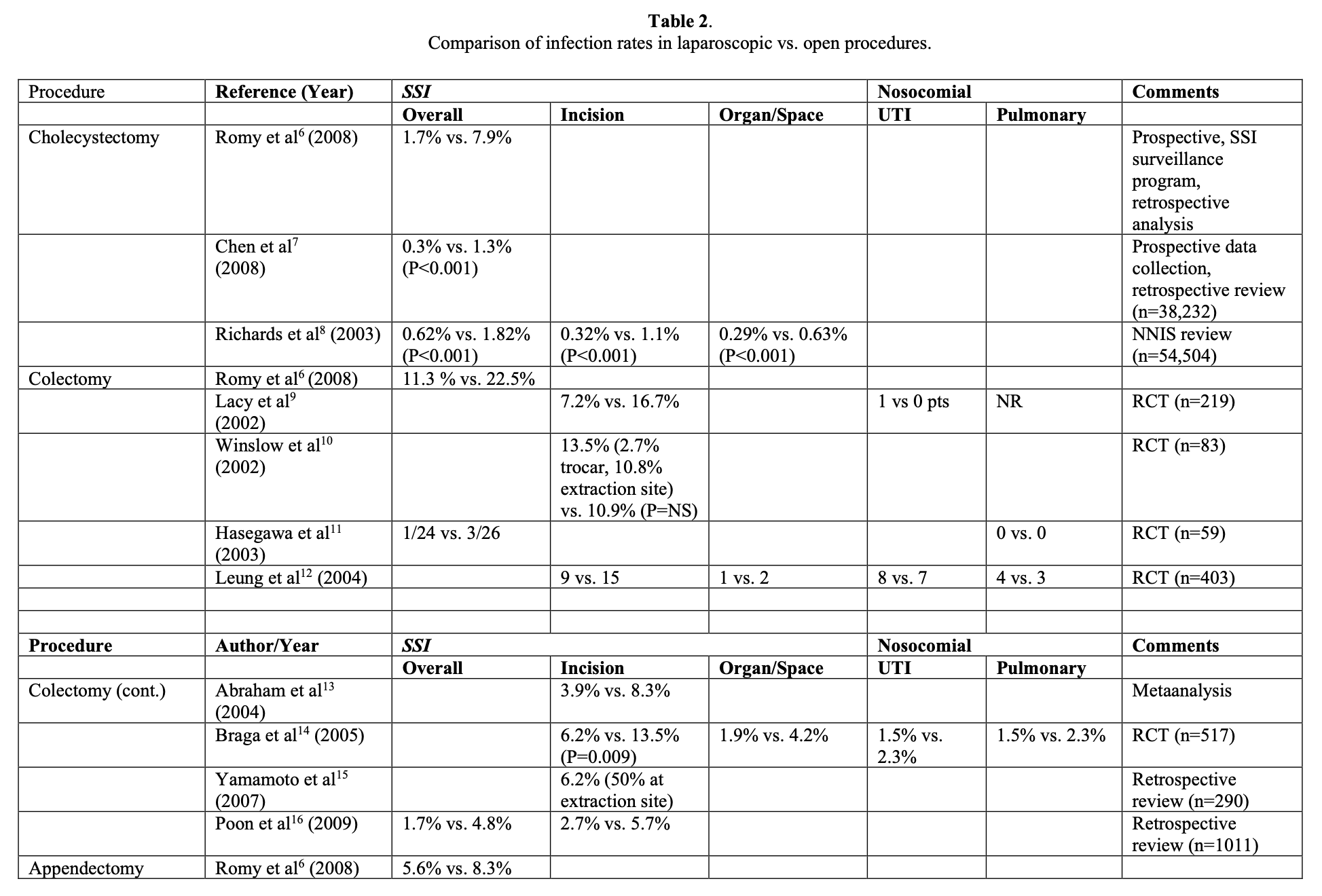
Laparoscopic surgery also reduces the risk of other nosocomial infections. The incidence of UTI and pulmonary infections following minimally invasive procedures compared with open procedures range from 0.7% vs. 2% and 1.5% vs. 5%, respectively.8,32
PREVENTION OF SSI
Utilizing known infection prophylaxis measures is best surgical practice and much more preferable than dealing with the morbidity of surgical-site infection. The majority of the published literature reports on the use of prophylactic antibiotics in open surgery.
Nevertheless, prevention of surgical-site infection in laparoscopic procedures is very similar to that of open surgery. In addition to prophylactic antibiotic administration, a variety of interventions specifically address prevention of surgical-site infection in laparoscopy.
Preoperative Measures
Preoperative interventions that may reduce SSI include preoperative antiseptic showering and clipping rather than shaving hair at the operative site. Although preoperative hair removal is surgical dogma, it is often unnecessary to successfully complete a laparoscopic procedure. Proper techniques for patient skin preparation, surgical team member hand/forearm antisepsis, draping of the site, and gowning/gloving should be routinely used in laparoscopic procedures.
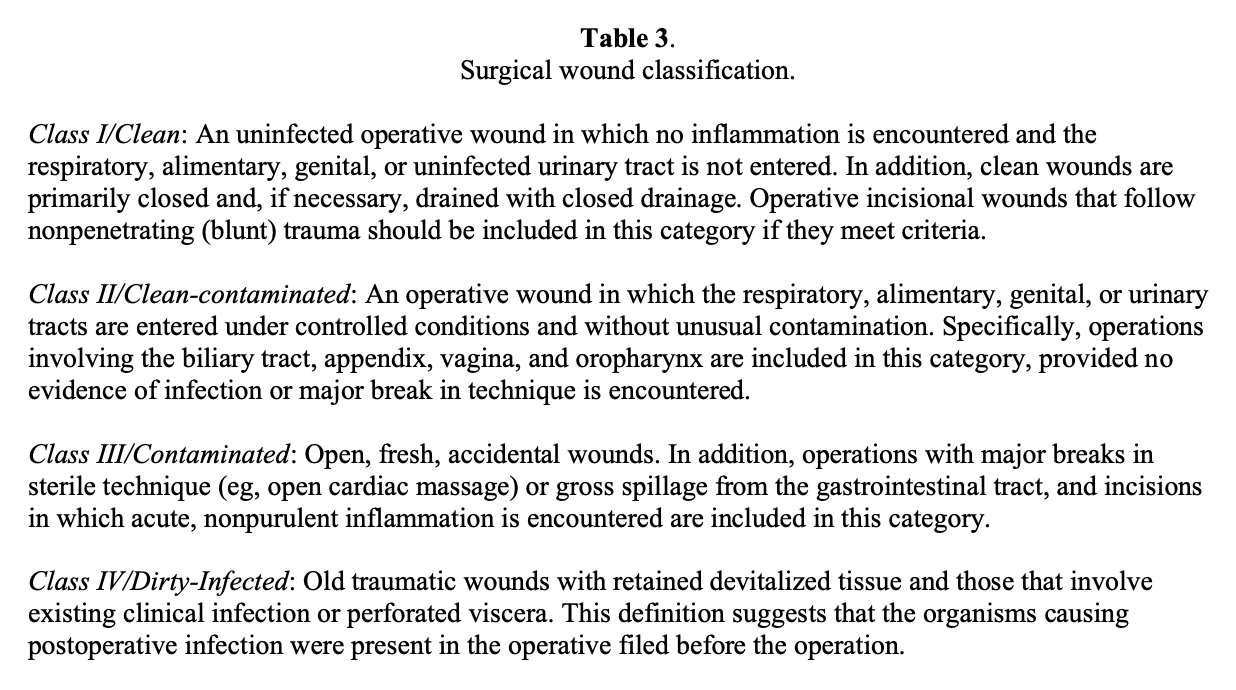
Preoperative prophylactic antibiotics should be utilized according to the classification of the surgical wound (Table 3). Prophylactic antibiotics are unnecessary in clean laparoscopic procedures, such as antireflux surgery, adrenalectomy, and splenectomy.
Interestingly, evidence is not sufficient to determine whether the use of antibiotics for laparoscopic procedures utilizing mesh prostheses reduces the incidence of mesh infection.33 However, given the complexity of treating mesh infection, the small risk of administering prophylactic antibiotics (particularly in laparoscopic ventral hernia repair) is recommended until randomized controlled studies address this issue. For clean- contaminated laparoscopic procedures (ie, colectomy, gastric bypass) antibiotics should be utilized. In regards to uncomplicated laparoscopic cholecystectomy, several trials have demonstrated that no difference exists in SSI rates when preoperative antibiotics are given, making their use unnecessary.34-43
Intraoperative Measures
Several intraoperative technical considerations have been studied in laparoscopic surgery in efforts to reduce surgical-site infection. Surgical drains are occasionally utilized in cholecystectomy when there is concern for possible fluid accumulation, such as bile or blood at the operative site. In theory, abdominal fluid collections may harbor bacterial growth; however, the routine use of drains in uncomplicated laparoscopic cholecystectomy increases infection rate and should not be used.44
Skin adhesives are an attractive option for trocar-site closure in laparoscopic surgery due to their speed and ease of use. They are equivalent to suture closure in terms of superficial surgical-site infection rates.45-48 Therefore, the use of either suture or skin adhesives for trocar-site skin closure is appropriate.
Plastic wound protectors are commonly used in laparoscopic colectomy. Their use does not necessarily decrease the incidence of surgical-site infection in laparoscopic-assisted colectomy.49 However, wound protectors do facilitate exposure and may protect against cancer recurrence in the wound. There is currently not enough literature to support routine use of these devices simply to reduce the risk of surgical-site infections.
Antibiotic-impregnated surgical incise drapes are occasionally used in laparoscopic hernia surgery with the goal of preventing surgical-site infections especially mesh infections. The theory is that despite a sterile surgical prep of the abdominal wall, adding an additional barrier that prevents contact of the mesh with the skin will reduce the incidence of contaminating the mesh and reduce mesh infection rates. Reported infection rates in nonlaparoscopic cases utilizing incise drapes have produced mixed results.50-57 Interestingly, a large database review of both laparoscopic and open ventral hernia repair with mesh conducted at the University of Virginia Health System demonstrated no difference in either surgical-site or mesh-infection rates with the use of these drapes.57 Despite the lack of strong evidence to support their use, there is virtually no risk from using these devices other than local skin reaction, and many surgeons find them useful for securing the operative site towels and drapes.
Some studies have specifically reported on techniques to reduce SSI after laparoscopic appendectomy. One area of interest is utilizing extraction bags to retrieve a markedly inflamed or perforated appendix from the peritoneal cavity. There is some evidence to support this practice in terms of reducing wound infections.58 Copious laparoscopic peritoneal irrigation and specimen retrieval through a 12-mm trocar is also suggested following appendectomy, but lacks strong evidence that it reduces SSI.59 Interestingly, several studies have demonstrated reduced rates of incisional SSI but equivalent rates of intraabdominal abscess with the use of endoscopic staplers rather than endoloops to secure the base of the appendix.60-63
Without larger randomized trials demonstrating superiority of these various techniques in reducing infection rates, the decision to utilize these intraoperative measures usually depends on surgeon preference, experience, and training, and operative time, cost, and equipment availability.
Postoperative Measures
There is some evidence that unconventional use of antibiotics in laparoscopic surgery may decrease the incidence of surgical-site infection. One trial of 48 laparoscopic cholecystectomy patients demonstrated that the use of topical rifamycin applied to the umbilical trocar incision decreased umbilical pain, inflammation, dehiscence, and incisional hernia within 60 postoperative days.64 An interesting review of 65 laparoscopic ventral hernia repairs reported that the use of a 7-day course of postoperative oral cephalosporins or fluoroquinolones in addition to preoperative intravenous prophylactic antibiotics decreased the rate of seroma-related cellulitis compared with preoperative antibiotics alone.65 That review also documented 2 cases of seroma-related cellulitis that developed into mesh infections requiring mesh removal.
DIAGNOSIS AND TREATMENT OF SSI
Superficial Incisional SSI
By definition, superficial incisional SSI involves only the skin and subcutaneous tissue and occurs within 30 days after the operation. Purulent drainage, positive fluid, or tissue cultures, pain or tenderness, localized swelling, redness, or heat are characteristic.1 Drainage and local wound care are usually sufficient treatment. Antibiotics may also be considered in severe cases or immunocompromised patients.
Deep Incisional SSI
Deep incisional SSI involves the fascia or muscle layers of the incision and also occurs within 30 days after the operation unless an implant was used. If an implant was used and the infection appears to be related to the operation, then a 1-year time frame is used.
Purulent drainage from the deep incision (but not from the organ space), fever, localized pain or tenderness, or wound dehiscence may be identified. An abscess or other evidence of infection found on reoperation, histopathologic, or radiologic examination may also indicate deep incisional infection.1 Deep incisional SSI often requires a more definitive drainage or debridement (or implant removal) in the operating room and systemic antibiotics for successful eradication.
Organ/Space SSI
Organ/space SSI is defined by infection that involves any part of the anatomy (eg, organs or spaces), other than the incision, which was opened or manipulated during and operation. These types of SSI also occur within 30 days after the operation unless an implant was used, in which case, a 1-year time frame is used. In addition, one of the following criteria must be present: purulent drainage from a drain that is placed through a stab wound into the organ/space, or organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space, or an abscess or other evidence of infection involving the organ/space that is found on direct examination, during reoperation, or by histopathologic or radiologic examination.1 The optimal treatment of laparoscopic-related organ/space SSI is similar to open surgery and typically requires laparoscopic, open, or percutaneous drainage and systemic antibiotics.
MESH INFECTION
Epidemiology
Mesh infection is a rare but dreaded complication in laparoscopic hernia surgery. The incidence in laparoscopic inguinal hernia repair is only 0% to 1%.25-28 In laparoscopic ventral hernia repair, the incidence of mesh infection is 0% to 1.5%.18-24,66-68 The most common organisms associated with mesh infections are Staphylococcus aureus [including methicillin-resistant Staphylococcus aureus (MRSA)], Streptococcus spp., Gram-negative bacteria (mainly Enterobacteriaceae), and anaerobic bacteria (including Peptostreptococcus spp.).69-71
Mesh Characteristics
Several types of prosthetic material have been used in both laparoscopic inguinal and ventral hernia repair. Typically, permanent, synthetic mesh is utilized. Polypropylene varieties are commonly used in inguinal hernia repair. In ventral hernia repair, expanded polytetrafluoroethylene (ePTFE)-containing mesh products are commonly used because of less risk of adhesion and fistula formation. Biologic grafts are occasionally utilized in laparoscopic ventral hernia repair, particularly in potentially contaminated or contaminated situations.72
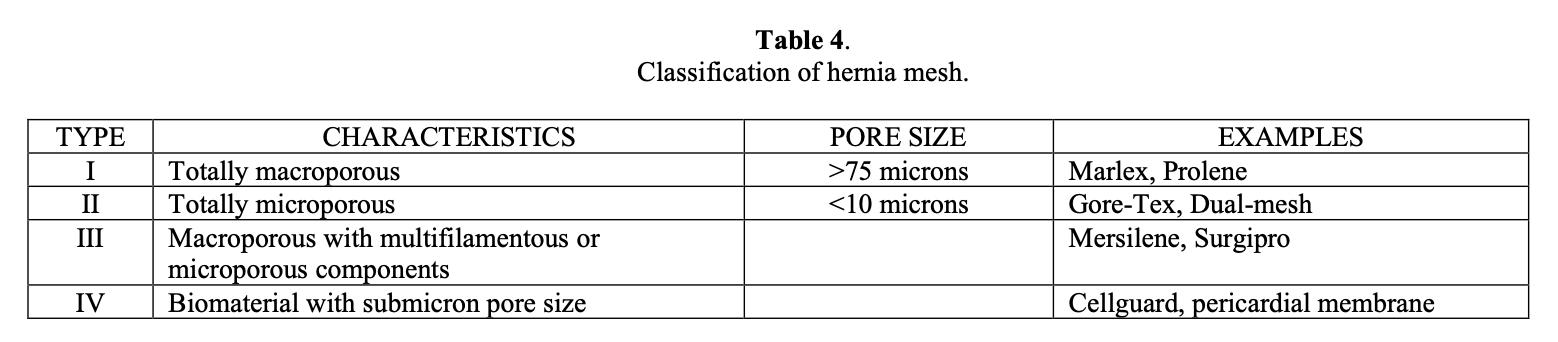
All mesh varieties incite some degree of inflammatory foreign body response by the host. However, the risk of mesh infection may differ based on the pore size of the mesh (Table 4). Macroporous mesh has larger pores and allows macrophages to permeate the mesh as well as fibroplasia and angiogenesis to occur. In contrast, mesh products with microporous constructs are more likely to become infected in the setting of contamination.73 Although there are not sufficient clinical trials in laparoscopic hernia repair to conclude superiority of the various prosthetic devices or biologic grafts in regards to infection risk, the available data and individual patient risk factors should be considered when performing laparoscopic hernia repair.
Prevention of Mesh Infection
Several strategies are useful in decreasing the incidence of mesh infection in laparoscopic hernia repair. Meticulous hemostasis, delicate tissue handling, and strict sterile technique are time-honored principles of surgery and must be utilized in all laparoscopic hernia repairs. Preoperative systemic parenteral antibiotics should be administered in both laparoscopic inguinal and ventral hernia repairs. A single dose of antibiotic is effective in reducing the incidence of infection in both open inguinal and ventral hernia repair.74-78 The use of topical antibiotic agents applied directly to the surgical wound to prevent mesh infection is controversial. There have been mixed results regarding the effectiveness of this approach.79,80 ePTFE impregnated with antibiotics has been shown in laboratory studies to minimize bacterial adherence.81,82 Antibiotic-coated mesh may reduce the risk of mesh infection but has never been demonstrated in a clinical trial.
Diagnosis of Mesh Infection
Mesh infections can occur within a few days up to several years after hernia repair. Early mesh infection is manifested by fever, pain, swelling, and drainage from surgical incisions including trocar sites. Lysis of intraabdominal adhesions is commonly required in laparoscopic ventral hernia repair; therefore, accidental enterotomy must be ruled out when signs of infection are present within the first few postoperative days.
Late mesh infection presents as an abdominal wall abscess or a chronic draining sinus tract. Late mesh infection should raise concern for the possibility of an enteric fistula to the mesh. Transient bacteremia may lead to seeding of the mesh and result in late infection as well.
Seroma, hematoma, hernia recurrence, and mesh-related neuralgia must be ruled out as causes of postoperative pain and swelling following laparoscopic hernia repair. Typically, these entities do not elicit postoperative fever but do have pain and swelling. Laboratory testing and diagnostic imaging are useful in detecting mesh infection. Laboratory findings of leukocytosis, elevated sedimentation rate, and elevated C-reactive protein levels indicate systemic inflammation and are consistent with mesh infection. Ultrasound or computed tomography studies may differentiate recurrent hernia from mesh infection but may not provide enough information to definitively characterize whether a fluid collection around a mesh implant is a seroma, hematoma, or infection. Percutaneous fluid sampling with microbiological evaluation confirms the diagnosis in this setting. The presence of enteric pathogens in the fluid suggests a fistula to the mesh and is of paramount importance in dictating subsequent surgical treatment.
Treatment of Mesh Infection
The treatment of mesh infection following laparoscopic hernia repair is not well studied because of the low incidence. Therefore, treatment is based on experience with mesh infection following open inguinal and ventral hernia repair. The treatment should be individualized based on several factors including the extent of the infection, type and location of the mesh, and complexity of the infection.
In general, intravenous antibiotics and mesh excision are the mainstays of treatment. A first-generation cephalosporin or vancomycin should be used unless there is a suspicion of involvement of enteric organisms. If there is a suspicion of enteric-mesh fistula, then broad-spectrum antibiotics should be given. The severity and extent of the infection and the extent of surgical debridement dictate the length of antibiotic treatment. The antibiotic duration may be from 1 week to 8 weeks. Antibiotics alone have been effective in a limited number of cases.83,84 Occasionally, long-term suppressive antibiotic therapy is used if mesh excision is incomplete.
Some degree of mesh debridement is usually necessary. Because Staphylococcus organisms are known to produce a biofilm on prosthetic devices and most mesh implants develop a thick, fibrous capsule around them as a result of the host’s inflammatory response, antibiotic penetration into host tissue around the mesh is impaired and results in poor contact with bacteria cell wall.69,85 The result is the relative ineffectiveness of antibiotics alone in treating mesh infection. Therefore, complete mesh excision is commonly required.83,86
Although complete mesh removal is very successful in regards to treating infection, that approach results in significant morbidity. Complete mesh removal for infected ventral hernia mesh frequently results in a large open abdominal wall defect. The residual fascial defect can be repaired with a variety of techniques including primary fascial closure, implanting biologic mesh or absorbable mesh, or component separation techniques.
Complex local wound care (often with an open abdomen) is typically necessary. In the case of an open abdomen, exposed viscera are at risk of fistula formation. Occasionally, split-thickness skin grafting is required to heal the open wound. As a result of the infection and large residual defect, there is a high recurrence rate.83,86-89
Because of the significant morbidity associated with complete mesh excision, attempts at less aggressive surgical management may be considered. Serial wound debridement combined with copious saline irrigation or drainage has been attempted with some success.90,91 Incision and drainage with limited mesh excision combined with negative pressure wound therapy has been somewhat promising.92,93 Percutaneous drainage with and without antibiotic irrigation has also been reported in a small number of cases.93,94 However, these limited attempts to salvage infected mesh often result in chronic sinus and fistula formation that ultimately lead to mesh removal.95
References
- Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR; The Hospital Infection Control Practices Advisory Committee. Guideline for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-278.
- Owens CD, Stoessel K. Surgical site infections: epidemiology, microbiology, and prevention. J Hosp Infect. 2008;70 Suppl 2:3-10.
- Boni L, Benevento A, Rovera F, et al. Infective complications in laparoscopic surgery. Surg Infect (Larchmt). 2006;7 Suppl 2:S109-11.
- Gaynes RP, Culver DH, Horan TC, et al. Surgical site infection (SSI) rates in the United States, 1992-1998: the national nosocomial infections surveillance system basic SSI risk index. Clin Infect Dis. 2001;33 Suppl 2:S69-77.
- Imai E, Ueda M, Kanao K, et al. Surgical site infection risk factors identified by multivariate analysis for patient undergoing laparoscopic, open colon, and gastric surgery. Am J Infect Control. 2008;36:727-731.
- Romy S, Eisenring MC, Bettschart V, et al. Laparoscope use and surgical site infections in digestive surgery. Ann Surg. 2008;247:627-32.
- Chen LF, Anderson DJ, Hartwig MG, et al. Surgical site infections after laparoscopic and open cholecystectomies in community hospitals. Infect Control Hosp Epidemiol. 2008;29:92-94.
- Richards C, Edwards J, Culver D, et al. Does using a laparoscopic approach to cholecystectomy decrease the risk of surgical site infection? Ann Surg. 2003;237:358- 362.
- Lacy AM, García-Valedcasas JC, Delgado S, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomized trial. 2002;359:2224-2229.
- Winslow ER, Fleshman JW, Birnbaum EH, Brunt LM. Wound complications of laparoscopic vs open colectomy. Surg Endosc. 2002;16:420-425.
- Hasegawa H, Kabeshima Y, Watanabe M, et al. Randomized controlled trial of laparoscopic versus open colectomy for advanced colorectal cancer. Surg Endosc. 2003;17:636-640.
- Leung KL, Kwok SP, Lam SC, et al. Laparoscopic resection of rectosigmoid carcinoma: prospective randomised trial. 2004;363:1187-1192.
- Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resection for colorectal cancer. Br J Surg. 2004;91:1111-1124.
- Braga M, Vignali A, Zuliani W, et al. Laparoscopic versus open colorectal surgery: cost-benefit analysis in a single-center randomized trial. Ann Surg. 2005;242:890-895.
- Yamamoto S, Fujita S, Akasu T, et al. Wound infection after elective laparoscopic surgery for colorectal carcinoma. Surg Endosc. 2007;21:2248-2252.
- Poon JT, Law WL, Wong IW, et al. Impact of laparoscopic colorectal resection on surgical site infection. Ann Surg. 2009;249:77-81.
- Sauerland S, Lefering R, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev. 2004;4:CD001546.
- Forbes SS, Eskicioglu C, McLeod RS, Okrainec A. Meta-analysis of randomized controlled trials comparing open and laparoscopic ventral and incisional hernia repair with mesh. Br J Surg. 2009;96:851-858.
- Pring CM, Tran V, O’Rourke N, Martin IJ. Laparoscopic versus open ventral hernia repair: a randomized controlled trial. Aust N Z J Surg. 2008;78:903-906.
- Carbajo MA, Martín del Olmo JC, Blanco JI, et al. Laparoscopic treatment vs open surgery in the solution of major incisional and abdominal wall hernias with mesh. Surg Endosc. 1999;13:250-252.
- Misra MC, Bansal VK, Kulkarni MP, Pawar DK. Comparison of laparoscopic and open repair of incisional and primary ventral hernia: results of a prospective randomized study. Surg Endosc. 2006;20:1839-1845.
- Barbaros U, Asoglu O, Seven R, et al. The comparison of laparoscopic and open ventral hernia repairs: a prospective randomized study. Hernia. 2007;11:51-56.
- Olmi S, Scaini A, Cesana GC, et al. Laparoscopic versus open incisional hernia repair. Surg Endosc. 2007;21:555-559.
- Navarra G, Musolino C, DeMarco ML, et al. Retromuscular sutured incisional hernia repair: a randomized controlled trial to compare open and laparoscopic approach. Surg Laparosc Endosc Percutan Tech. 2007;17:86-90.
- Fitzgibbons RJ, Camps J, Cornet DA, et al. Laparoscopic inguinal herniorrhaphy: results of a multicenter trial. Ann Surg. 1995;221:3-13.
- Liem MSL, van der Graaf Y, van Steensel CJ, et al. Comparison of conventional anterior surgery and laparoscopic surgery for inguinal hernia repair. N Engl J Med 1995;336:1541-1547.
- Andersson B, Hallén M, Leveau P, et al. Laparoscopic extraperitoneal inguinal hernia repair versus open mesh repair: a prospective randomized controlled trial. Surg 2003;133:464-472.
- Neumayer L, Giobbie-Hurder A, Jonasson O, et al. Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 2004;350:1819-1827.
- Biscione FM, Couto RC, Pedrosa TM, Neto MC. Factors influencing the risk of surgical site infection following diagnostic exploration of the abdominal cavity. J Infect. 2007;55:317-323.
- Balague Ponz C, Trias M. Laparoscopic surgery and surgical infection. J Chemother. 2001;13:17-22.
- Targarona EM, Balague C, Knook MM, Trias M. Laparascopic surgery and surgical infection. Br J Surg. 2000;87:536-544.
- Shindholimath VV, Seenu V, Parshad R, et al. Factors influencing wound infection following laparoscopic cholecystectomy. Trop Gastroenterol. 2003;24:90-92.
- Goldfaden A, Birkmeyer JD. Evidence-based practice in laparoscopic surgery: perioperative care. Surg Innov. 2005;12:51-61.
- Illig KA, Schmidt E, Cavanaugh J, et al. Are prophylactic antibiotics required for elective laparoscopic cholecystectomy? J Am Coll Surg. 1997;184:353-356.
- Dobay KJ, Freier DT, Albear P. The absent role of prophylactic antibiotics in low- risk patients undergoing laparoscopic cholecystectomy. Am Surg. 1999;65:226-228.
- Higgins A, London J, Charland S, et al. Prophylactic antibiotics for elective laparoscopic cholecystectomy: are they necessary? Arch Surg. 1999;134:611-613.
- Tocchi A, Lepre L, Costa G, et al. The need for antibiotic prophylaxis in elective laparoscopic cholecystectomy: a prospective randomized study. Arch Surg. 2000;135:67- 70.
- Mahatharadol V. A reevaluation of antibiotic prophylaxis in laparoscopic cholecystectomy: a randomized controlled trial. J Med Assoc Thai. 2001;84:105-108.
- Koc M, Zulfikaroglu B, Kece C, Ozalp N. A prospective randomized study of prophylactic antibiotics in elective laparoscopic cholecystectomy. Surg Endosc. 2003;17:1716-1718.
- Kuthe SA, Kaman L, Verma GR, Singh R. Evaluation of the role of prophylactic antibiotics in elective laparoscopic cholecystectomy: a prospective randomized trial. Trop Gastroenterol. 2006;27:54-57.
- Chang WT, Lee KT, Chuang SC, et al. The impact of prophylactic antibiotics on postoperative infection complication in elective laparoscopic cholecystectomy: a prospective randomized study. Am J Surg. 2006;191:721-725.
- Choudhary A, Bechtold ML, Puli SR, et al. Role of prophylactic antibiotics in laparoscopic cholecystectomy: a meta-analysis. J Gastrointst Surg. 2008;12:1847-1853.
- Yildiz B, Abbasoglu O, Tirnaksiz B, et al. Determinants of postoperative infection after laparoscopic cholecystectomy. Hepatogastroenterology. 2009;56:589-592.
- Gurusamy KS, Samraj K, Mullerat P, Davidson BR. Routine abdominal drainage for uncomplicated laparoscopic cholecystectomy. Cochrane Database Syst Rev. 2007;4:CD006004.
- Matin SF. Prospective randomized trial of skin adhesive versus sutures for closure of 217 laparoscopic port-site incisions. J Am Coll Surg. 2003;196:845-853.
- Jallali N, Haji A, Watson CJ. A prospective randomized trial comparing 2-octyl cyanoacrylate to conventional suturing of laparoscopic cholecystectomy incisions. J Laparoendosc Adv Surg Tech A. 2004;14:209-211.
- Sebesta MJ, Bishoff JT. Octylcyanoacrylate skin closure in laparoscopy. JSLS. 2004;8:9-14.
- Sajid MS, Siddiqui MR, Khan MA, Baig MK. Meta-analysis of skin adhesives versus sutures in closure of laparoscopic port-site wounds. Surg Endosc. 2009;23:1191- 1197.
- Kercher KW, Nguyen TH, Harold KL, et al. Plastic wound protectors do not affect wound infection rates following laparoscopic-assisted colectomy. Surg Endosc. 2004;18:148-151.
- Rittenbury MS, Hume DM, Hench ME. A clinical bacteriologic evaluation of surgical antiseptics and a plastic skin drape. Surg Gynecol Obstet. 1964;119:568-574.
- French ML, Witzen HE, Ritter MA. The plastic surgical adhesive drape: an evaluation of its efficacy as a microbial barrier. Ann Surg. 1976;184:46-50.
- Geelhoed GW, Sharpe K, Simon GL. A comparative study of surgical skin preparation methods. Surg Gynecol Obstet.1983;157:265-268.
- Fairclough JA, Johnson D, Mackie I. The prevention of wound contamination by skin organisms by the pre-operative application of an iodophor-impregnated plastic adhesive drape. J Int Med Res. 1986;14:105-109.
- Dewan PA, Van Rij AM, Robinson RG, et al. The use of an iodophor-impregnated plastic incise drape in abdominal surgery: a controlled clinical trial. Aust N Z J Surg. 1987;57:859-863.
- Chiu KY, Lau SK, Fung B, et al. Plastic adhesive drapes and wound infection after hip fracture surgery. Aust N Z J Surg. 1993;63:798-801.
- Yoshimura Y, Kubo S, Hirohashi K, et al. Plastic iodophor drape during liver surgery operative use of the iodophor-impregnated adhesive drape to prevent wound infection during high risk surgery. World J Surg. 2003;27:685-688.
- Swenson BR, Camp TR, Mulloy DP, Sawyer RG. Antimicrobial-impregnated surgical incise drapes in the prevention of mesh infection after ventral hernia repair. Surg Infect (Larchmt). 2008;9:23-32.
- Khan MN, Fayyad T, Cecil TD, Moran BJ. Laparoscopic versus open appendectomy: the risk of postoperative infectious complications. JSLS. 2007;11:363-367.
- Hussain A, Mahmood H, Nicholls J, El-Hasani S. Prevention of intra-abdominal abscess following laparoscopic appendicectomy for perforated appendicitis: a prospective study. Int J Surg. 2008;6:374-377.
- Ortega AE, Hunter JG, Peters JH, et al. A prospective, randomized comparison of laparoscopic appendectomy with open appendectomy. Am J Surg. 1995;169:208-213.
- Shalaby R, Arnos A, Desoky A, Samaha AH. Laparoscopic appendectomy in children: evaluation of different techniques. Surg Laparosc Endosc Percutan Tech. 2001;11:22-27.
- Kazemier G, in’t Hof KH, Saad S, et al. Securing the appendiceal stump in laparoscopic appendectomy: evidence for routine stapling? Surg Endosc. 2006;20:1473- 1476.
- Sajid MS, Rimple J, Cheek E, Baig MK. Use of endo-GIA versus endo-loop for securing the appendicular stump in laparoscopic appendectomy: a systematic Surg Laparosc Endosc Percutan Tech. 2009;19:11-15.
- Neri V, Fersini A, Ambrosi A, et al. Umbilical port-site complications in laparoscopic cholecystectomy: role of topical antibiotic therapy. JSLS. 2008;12:126-132.
- Edwards C, Angstadt J, Whipple O, Grau R. Laparoscopic ventral hernia repair: postoperative antibiotics decrease incidence of seroma-related cellulitis. Am Surg. 2005;71:931-935.
- Asencio F, Aguiló J, Peiró S, et al. Open randomized trial of laparoscopic versus open incisional hernia repair. Surg Endosc. 2009;23:1441-1448.
- Heniford BT, Park A, Ramshaw BJ, Voeller G. Laparoscopic repair of ventral hernias: nine years’ experience in 850 consecutive hernias. Ann Surg. 2003;238:391-399.
- Pierce RA, Spitler JA, Frisella MM, et al. Pooled data analysis of laparoscopic open hernia repair: 14 years of patient data accrual. Surg Endosc. 2007;21:378-386.
- Falagas ME, Kasiakou SK. Mesh-related infections after hernia repair surgery. Clin Microbiol Infect. 2005;11:3-8.
- Cobb WS, Harris JB, Lokey JS, et al. Incisional herniorrhaphy with intraperitoneal composite mesh: a report of 95 cases. Am Surg. 2003;69:784-787.
- Taylor SG, O’Dwyer PJ. Chronic groin sepsis following tension-free inguinal hernioplasty. Br J Surg. 1999;86:562-565.
- Franklin ME, Trevino JM, Portillo G, et al. The use of porcine small intestinal submucosa as a prosthetic material for laparoscopic hernia repair in infected and potentially contaminated fields: long-term follow-up. Surg Endosc. 2008;22:1941-1946.
- Amid PK. Classification of biomaterials and their related complications in abdominal wall hernia surgery. 1997;1:15-21.
- Yerdel MA, Akin EB, Dolalan S, et al. Effect of single-dose prophylactic ampicillin and sulbactam on wound infection after tension-free inguinal hernia repair with polypropylene mesh: the randomized, double-blind, prospective trial. Ann Surg. 2001;233:26-33.
- Rios A, Rodriguez JM, Munitiz V, et al. Antibiotic prophylaxis in incisional hernia repair using a prosthesis. 2001;5:148-152.
- Platt R, Zalenznik DF, Hopkins CC, et al. Perioperative antibiotic prophylaxis for herniorrhaphy and breast surgery. N Engl J Med. 1990;322:153-160.
- Abramov D, Jeroukhimov I, Yinnon AM, et al. Antibiotic prophylaxis in umbilical and incisional hernia repair: a prospective randomized study. Eur J Surg. 1996;162:945- 948.
- Celdrán A, Frieyro O, de la Pinta JC, et al. The role of prophylactic antibiotics on wound infection after mesh hernia repair under local anesthesia on an ambulatory basis. Hernia. 2004;8:20-22.
- Lazorthes F, Chiotasso P, Massip P, et al. Local antibiotic prophylaxis in inguinal hernia repair. Surg Gynecol Obstet. 1992;175:569-570.
- Troy MG, Dong QS, Dobrin PB, Hecht D. Do topical antibiotics provide improved prophylaxis against bacterial growth in the presence of polypropylene mesh? Am J Surg. 1996;171:391-393.
- Harrell AG, Novitsky YW, Kercher KW, et al. In vitro infectability of prosthetic mesh by methicillin-resistant Staphylococcus aureus. 2006;10:120-124.
- Carbonell AM, Matthews BD, Dréau D, et al. The susceptibility of prosthetic biomaterials to infection. Surg Endosc. 2005;19:430-435.
- LeBlanc KA, Whitaker JM, Cellanger DE, Rhynes VK. Laparoscopic incisional and ventral hernioplasty: lessons learned from 200 patients. Hernia. 2003;7:118-124.
- Bageacu S, Blanc P, Breton C, et al. Laparoscopic repair of incisional hernias. Surg Endosc. 2002;16:345-348.
- Buret A, Ward KH, Olson ME, Costerton JW. An in vivo model to study the pathobiology of infectious biofilms on biomaterial surfaces. J Biomed Mater Res. 1991;25:865-874.
- Rosen M, Brody F, Ponsky J, et al. Recurrence after laparoscopic ventral hernia repair. Surg Endosc. 2003;17:123-128.
- Heniford TB, Park A, Ramshaw BJ, Voeller G. Laparoscopic ventral and incisional hernia repair in 407 patients. J Am Coll Surg. 2000;190:645-650.
- Franklin ME, Dorman JP, Glass JL, et al. Laparoscopic ventral and incisional hernia repair. Surg Laparosc Endosc. 1998;8:294-299.
- Wright BE, Niskanen BD, Peterson DJ, et al. Laparoscopic ventral hernia repair: are there comparative advantages over traditional methods of repair? Am Surg. 2002;68:291- 296.
- Petersen S, Hence G, Freitag M, et al. Deep prosthesis infection in incisional hernia repair: predictive factors and clinical outcome. Eur J Surg. 2001;167:453-457.
- Kercher KW, Siing RF, Matthews BD, Heniford BT. Successful salvage of infected PTFE mesh after ventral hernia repair. Ostomy Wound Manage. 2002;48:40-42, 44-45.
- Steenvoorde P, de Roo RA, Oskam J, Neijenhuis P. Negative pressure wound therapy to treat peri-prosthetic methicillin-resistant Staphylococcus aureus infection after incisional herniorrhaphy. A case study and review of the literature. Ostomy Wound Manage. 2006;52:52-54.
- Paton BL, Novitsky YW, Zerey M, et al. Management of infections of polytetrafluoroethylene-based mesh. Surg Infect (Larchmt). 2007;8:337-341.
- Trunzo JA, Ponsky JL, Jin J, et al. A novel approach for salvaging infected prosthetic mesh after ventral hernia repair. Hernia. 2009;13:545-549.
- Jezupovs A, Mihelsons M. The analysis of infection after polypropylene mesh repair of abdominal wall hernia. World J Surg. 2006;30:2270-2278.