Odysseas Ath. Savvouras, Arathi Veeraswamy, James E. Carter
Pelvic pain is a debilitating condition, posing quality-of-life issues for the individual patient. Despite the passage of time and extensive investigation of this enigmatic disorder remains unknown .The disorder represents a major cause of gynecologic hospitalization in the United States, estimated to have exceeded billions of $ in in-patient health care costs in 2004 alone.2,3 In fact, CPP is considered the principal indication for approximately 20 percent of all hysterectomies performed for benign disease and at least 40 percent of all gynecological laparoscopies performed annually in the United States.27,28 The significant individual and public health concerns associated with pelvic underscore the importance of understanding its pathogenesis and focuses more on treatment of the symptomatology.
Laparoscopic surgery – Approximately one-third of outpatient laparoscopic surgical procedures in women are performed because of abdominal/pelvic pain.29 In large series, the type and frequency of laparoscopic findings in women with CPP were: no visible pathology (35%), endometriosis (33%), adhesions (24%), chronic PID (5%), ovarian cysts (3%), with occasional other diagnoses.30 The absence of visible pathology does not exclude a physical basis for the patient’s pain, but does exclude several common disorders which can be visualized at surgery (endometriosis, adnexal mass, adhesions, some uterine abnormalities, PID).
Laparoscopic uterosacral nerve ablation and presacral neurectomy are ancillary procedures meant to further decrease endometriosis-associated pelvic pain symptoms. Presacral neurectomy, involving cutting the T10-L1 sympathetic nerves on the anterior surface of the sacral bone and paracervical uterine denervation, involving transection of the uterosacral ligament at its attachment to the uterus along with cutting the above- mentioned sympathetic nerves and the S1S4 parasympathetic nerves, which transmit pain stimuli from the supravaginal region into the uterine cervix.1 Surgery for the treatment of peritoneal endometriosis includes several options: electrocoagulation, laser ablation, plasmajet or excision of the lesions, all of which have similar efficacy in the therapy of endometriosis-associated pelvic pain.24
Uterosacral transection was developed and popularized as an alternative to presacral neurectomy with Doyle’s vaginal approach, involving transection of the uterosacral ligaments.1 As described by Sutton and Whitelaw: Doyle would place a suture through the posterior lip of the cervix at the apex of the vagina and place traction on this suture to increase the distance of the cervix from the ureter.2 The attachments of the uterosacral ligaments to the cervix were then divided between Heaney clamps. To prevent re-growth of the dissected nerve trunks, the posterior leaf of the peritoneal incision was interposed between them. An abdominal approach was recommended if endometriosis was suspected or any gross pathology such as fibroids was felt. The pathological tissue was then excised. The ligaments were divided between two clamps and the ligaments sutured together with stainless steel sutures to the isthmus of the cervix in the midline about 1 cm higher than the original attachment. Doyle reported complete pain relief in 63 out of 73 cases (86%); 35 had primary dysmenorrhea (85.7% success) and 33 had secondary dysmenorrhea (86.8% success).
A more recent technique involves not separation and transection, but ablation of the uterosacral ligaments to achieve pain control. Lichtenand Bombard reported relief of incapacitating primary dysmenorrhea in nine of 11 patients (81%) who underwent laparoscopic uterosacral nerve ablation (LUNA) with no cure in the control group, which had only diagnostic laparoscopy.3 However, 1 year later, fewer than half the patients who originally expressed improvement were pain-free. Gurgan and colleagues reported that 17 of 23 patients had alleviation of dysmenorrhea, with a mean pain reduction of 33% based on pre-and postoperative pain scores.4 In a similar study, Sutton reported a 63% reduction from the initial average pain score.5
In a double-blind randomized, controlled trial of LUNA for women with chronic pelvic pain in the absence of endometriosis, Johnson reported a significant reduction in dysmenorrhea at 12-month follow-up.6 The median reduction on the visual analog scale (VAS) from baseline was 4.8 points for the LUNA group versus a reduction of 0.8 points for those who did not have LUNA. A total of 42.1% of the women experienced successful treatment for dysmenorrhea, defined as a 50% or greater reduction in VAS scores, versus 14.3% of those who did not undergo LUNA. There was no significant difference in pain scores in women with non-menstrual pelvic pain, deep dyspareunia, or dyschezia with no endometriosis who underwent LUNA versus those who did not undergo LUNA. The addition of LUNA to laparoscopic surgical treatment of endometriosis was not associated with a significant difference in pain outcome. Johnson concluded that LUNA is effective for dysmenorrhea in the absence of endometriosis and that there is no evidence for the effectiveness of LUNA for chronic pelvic pain without dysmenorrhea or for any type of pelvic pain associated with endometriosis.
Yen performed an elegant study involving the addition of LUNA to laparoscopic bipolar coagulation of the uterine vessels.7 This study, which was performed for women with uterine myomas and dysmenorrhea, involved 85 patients. Forty of the 41 women (97.6%) underwent successful laparoscopic bipolar coagulation of uterine vessels with LUNA. Forty-three of the 44 women (97.7%) assigned to laparoscopic bipolar coagulation of uterine vessels only underwent successful surgery. Eighty women completed the 1-, 3-, and 6-month follow-ups. The frequency and severity of postoperative pain were less in the group that had LUNA than in the group receiving coagulation of the uterine arteries only (P. 0.05). At 3 months, dysmenorrhea improved 84.2% in the LUNA group versus 61.9% for the group that did not have LUNA, and improved 92.1% versus 73.8% at 6- month follow-up. The reduction was more significant in the group that received LUNA than in the group that did not (P. 0.05). The results suggest that LUNA may decrease postoperative ischemic pain and improve dysmenorrhea associated with uterine myomas treated with laparoscopic bipolar coagulation of uterine vessels.
ANATOMY
Uterine nerve ablation involves the cauterization resulting in transection of the uterosacral ligaments close to their point of insertion into the cervix. The procedure interrupts pelvic afferent sensory nerve fibers of the Lee–Frankenhauser nerve plexus.8 According to Counseller and Craig, the Th10-L1 sympathetic nerves are included in the hypogastric nerve and run along the inferior vena cava and the sacral bone.8 They enter the pelvic cavity and run inside the uterosacral ligaments before ultimately entering the uterus. The parasympathetic nerves from S1-S4 are included in the nervi erigentes, and they run inside the uterosacral ligament for a short distance in the lateral part of the pelvis and then form ganglia on each side of the uterus (Frankenhauser ganglia). Johnson elegantly summarized the anatomy important for an understanding of the LUNA procedure.6 He pointed out that “the ideal neuroablative surgical procedure for pelvic pain would transect all afferent sensory fibers from all the pelvic organs and leave all other nerves unaffected.” Although pelvic neuroanatomy is complicated and still not completely understood, what is known makes it clear that no such “ideal neuroablative surgical procedure” exists (Figure 1). The body of the uterus is widely considered to be innervated only by sympathetic nerves.9 The cervix has predominantly parasympathetic (but also sympathetic) innervation. The afferent sensory nerves from both the uterus and cervix traverse the cervical division of the Lee–Frankenhauser plexus, which lies within and around the site of attachment of the uterosacral ligaments to the posterior aspect of the cervix.10,11
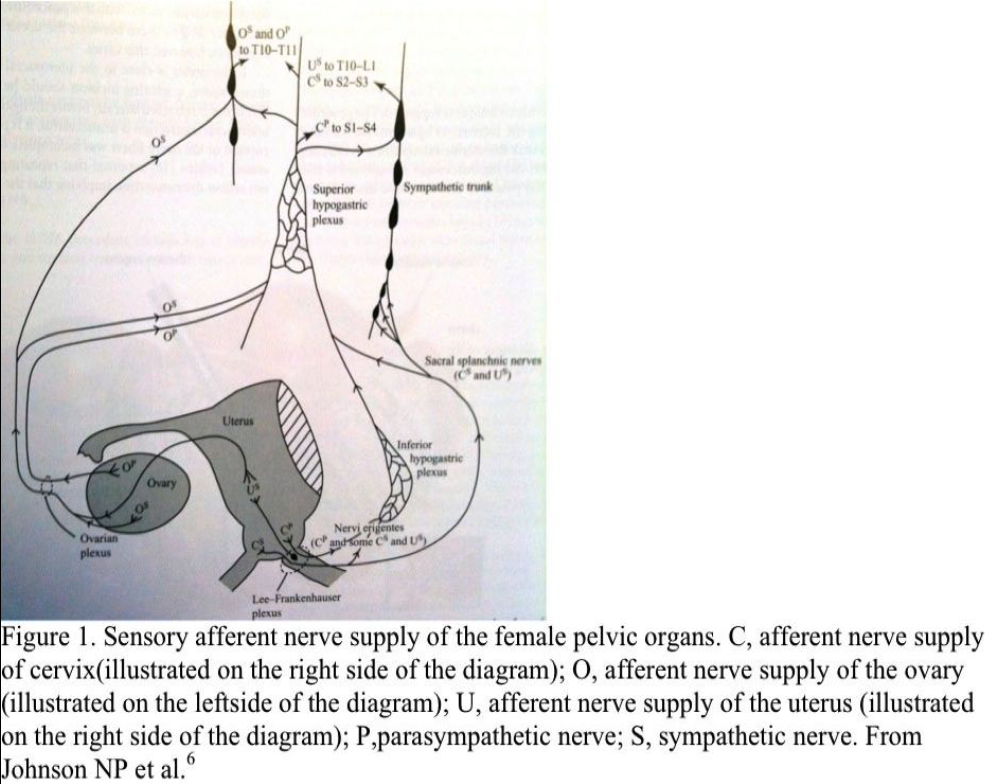
From the uterosacral ligaments, the parasympathetic afferent nerves reach the dorsal root ganglia of S1-S4 via the pelvic splanchnic nerves (nervi erigentes) and inferior hypogastric nerve plexus (also known as the pelvic plexus), and then the superior hypogastric nerve plexus (also known as the presacral nerve or hypogastric plexus).12 The sympathetic afferent nerves emerging from the Lee–Frankenhauser plexus accompany the uterine, iliac, and inferior mesenteric arteries to the sacral sympathetic trunk via the sacral splanchnic nerves, some of which bypass the superior hypogastric nerve plexus.
Afferent nerves accompany both parasympathetic and sympathetic nerves from the ovary. Pain fibers bypass the uterosacral ligament and course through corresponding plexuses to their cells of origin in the dorsal root ganglia (T10-T11). Some of the afferent nerves of the upper ovarian plexus course directly via the renal and aortic plexuses and bypass the presacral nerve.6 It is no surprise that LUNA has not been known to be an effective adjunct to laparoscopic surgical removal of endometriosis.6 The operation interrupts only some of the afferent sensory nerve fibers from the pelvis, and thus LUNA may be less effective for pelvic pain associated with more extensive pathology. Careful study of Figure 1 clarifies why transection of the Lee–Frankenhauser nerve plexus and LUNA could be particularly ineffective for pain arising from the ovary or adjacent tissues, as could be the case in ovarian or paraovarian endometriosis, because all ovarian afferent nerves bypass the Lee–Frankenhauser plexus and many of the pain fibers also bypass the presacral nerve. Without performing a periarterial sympathectomy of the iliac, inferior mesenteric, and ovarian vessels, a number of afferent fibers will always be left intact. It has been argued persuasively that the effectiveness of a LUNA procedure for endometriosisrelated pain could be due more to a debulking of endometriotic lesions. The most common site for endometriosis on the uterosacral ligament is the very site where the uterine nerve ablation is performed.13
Fujii et al. investigated the localization of nerves in the uterosacral ligament to determine the optimal site for uterosacral nerve ablation.14 In their study, they found that the largest number of nerve fiber bundles and nerve cells were located 1.65 to 3.30 cm distal to the site of attachment of the uterosacral ligament to the uterine cervix at a depth of 0.3 to 1.5 cm. A relatively large number of nerve fiber bundles were found in horizontal sections at a depth of 1.0 cm. They concluded that this area is the most appropriate region anatomically for resection of the uterosacral ligament for the purpose of blocking the pain pathway.
TECHNIQUE
A standard three-puncture technique is suggested. The procedure is performed by placing the uterosacral ligaments on stretch by anteverting the uterus with the uterine manipulator. A CO2 laser (40 to 60 W) or another cutting instrument is employed to transect the ligaments at the points of their insertion into the cervix using a vertical motion from medial to lateral (Figure 2).15
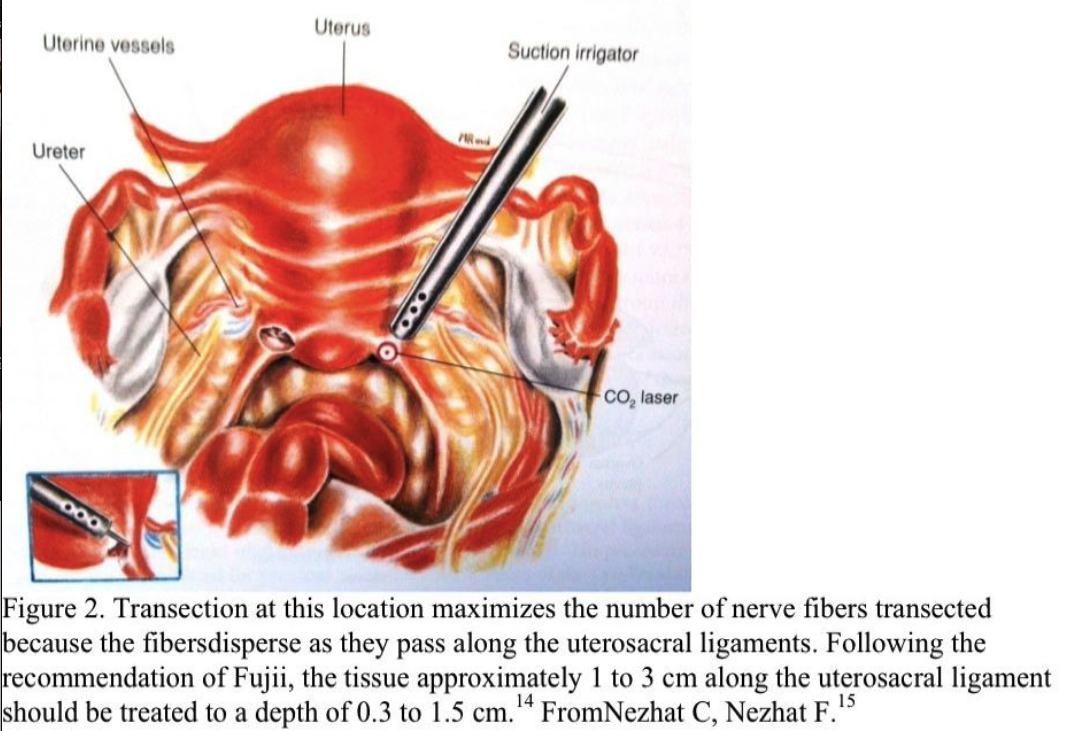
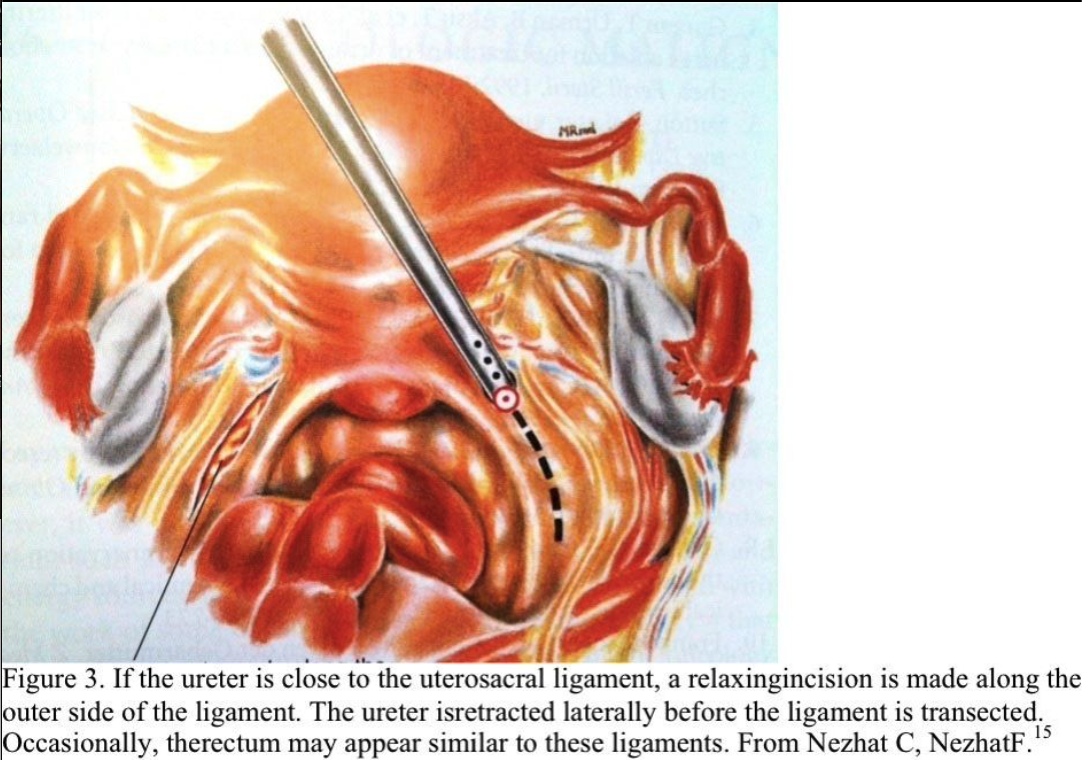
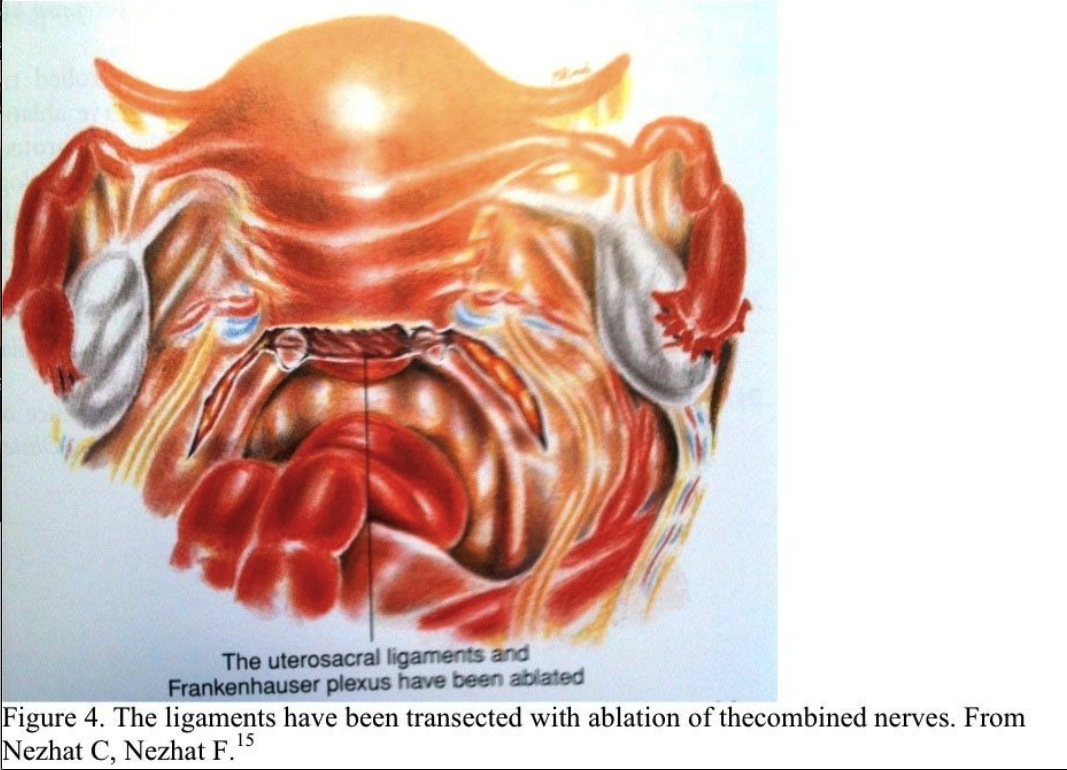
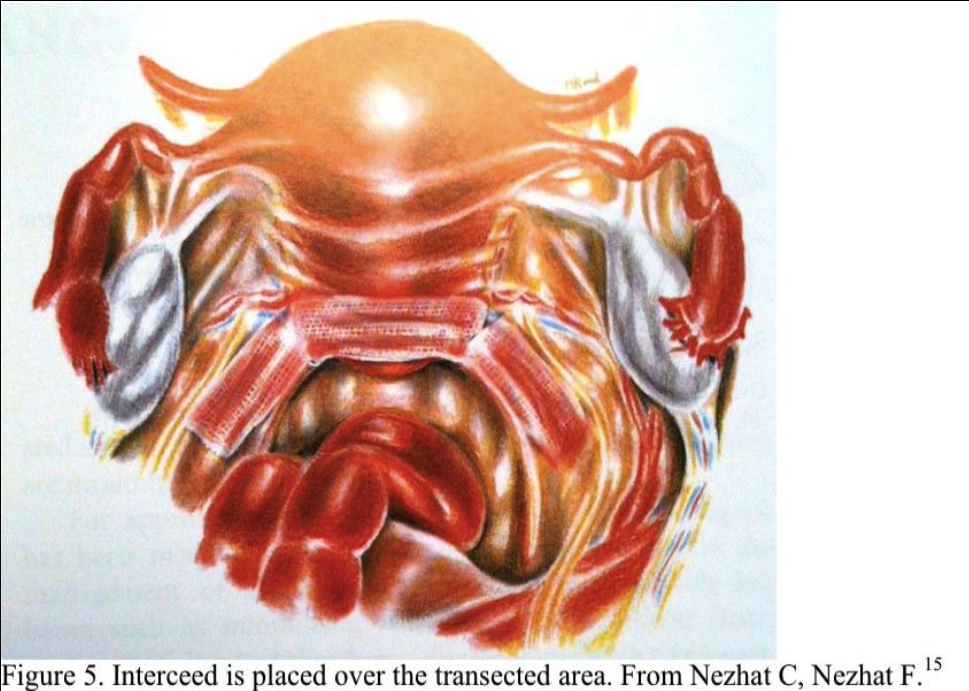
Following the recommendation of Fujii, the tissue located approximately 1 to 3 cm along the uterosacral ligament should be treated to a depth of 1.5 cm.14 This segment of the uterosacral ligament is close to the uterine vessels and ureter. The suction– irrigator serves as a backstop to make the uterosacral ligament more prominent and protect the ureter. A relaxing incision may be made along the outer side of the ligament to retract the ureter laterally before the ligament is transected (Figure 3). The blood vessels run along the medial aspect of the uterosacral ligament, and bleeding in this area must be controlled carefully because of the proximity of the ureter and rectum. Some gynecologists also vaporize a path along the base of the cervix between the uterosacral ligaments (Figure 4). Interceed (Gynecare) may be placed over the transected area (Figure 5).
If the uterosacral ligaments are difficult to identify, uterosacral transection is not recommended. When the uterosacral ligament is cut, a blood vessel inside it tends to bleed. To ascertain if this has occurred, uterine traction should be released and pneumoperitoneum should be decreased.
The direction of the ureter should be identified from the pelvic brim to the bladder because ureteral injury is a serious complication associated with this procedure.14 There is usually a distance of 2 to 3 cm between the ureter and the uterosacral ligaments; however, this varies.
If the ureter is close to the uterosacral ligaments, as mentioned above, a relaxing incision should be made as described.
The ureter is retracted laterally before the ligament is transected. If uterosacral transection is unsuccessful, it is presumed that interruption of the nerve fibers was incomplete or the nerves regenerated. Lichten reported that repeating the procedure did not relieve dysmenorrhea, implying that the course of the nerve fibers in these individuals may not be normal. Several patients with failed uterosacral transection have obtained relief from a subsequent presacral neurectomy.16
COMPLICATIONS
Complications of the LUNA procedure include loss of uterine support, adhesions, and ureteral transections, with loss of uterine support deserving special mention. Davis noted severe uterine prolapse in three young female soldiers during or after undergoing the rigors of airborne training.17
All three had previously undergone LUNA procedures. No other risk factors for uterine prolapse could be identified in these cases. He went on to state that although the etiology of uterine prolapse is complex, and no conclusions as to cause and effect can be made, these cases suggest that LUNA should be performed with caution on women whose occupation and lifestyle are associated with heavy physical labor or exercises producing marked increases in intra-abdominal pressure. Good reported on uterine prolapse after laparoscopic uterosacral nerve transection in women who had previous vaginal delivery.18
CONCLUSION
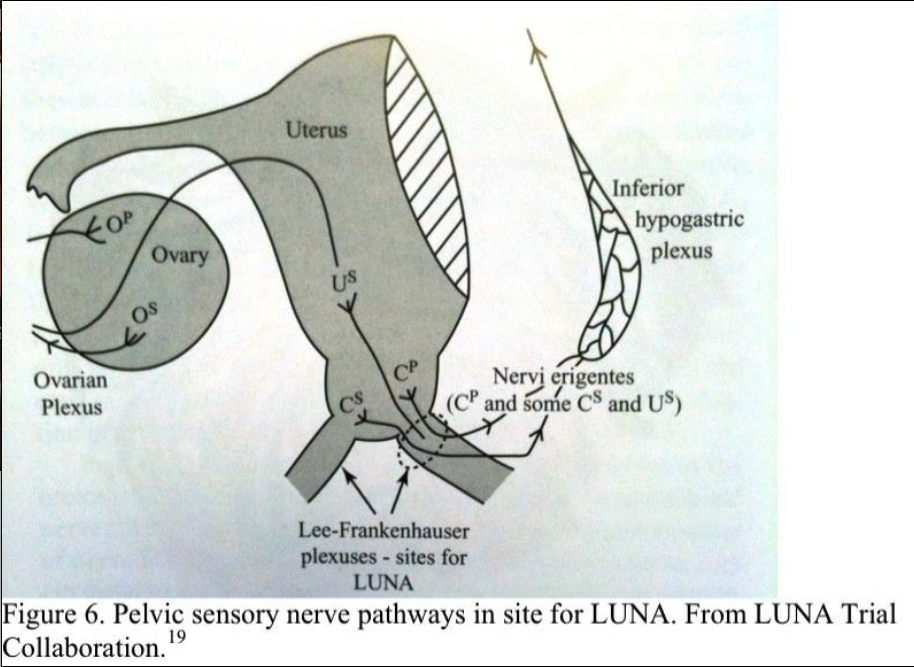
A randomized, controlled trial to assess the efficacy of LUNA in the treatment of chronic pelvic pain is ongoing through the LUNA trial collaborative study.19 The principal objective of this multicenter prospective randomized, controlled study is to test the hypothesis that LUNA alleviates pain and improves life quality in women with chronic pelvic pain and no pathology or mild endometriosis (American Fertility Society score .5). Patients in the study are randomized to either diagnostic laparoscopy with LUNA or to no pelvic denervation. The site for the LUNA in this study is the Lee–Frankenhauser plexus (Figure 6). Assessments are carried out in a blinded fashion, and the protocol calls for 12-month follow-up.
Latthe et al. reported that among clinicians, there is widespread variation in the practice and use of LUNA for treatment of chronic pelvic pain.20 Additionally, they found wide variation in beliefs about the effectiveness of the procedure for pelvic pain, ranging from substantial benefit to slight harm. The majority of respondents stated that LUNA would benefit patients in terms of improved VAS scores, but expectations regarding the level of benefit varied widely.
In a European survey, Latthe et al. found variation in methods of performing the LUNA procedure.21 Noting that recent anatomic studies have demonstrated that the greatest numbers of nerve fiber bundles are found some distance from the site of the attachment of uterosacral ligament to the cervix, there is some controversy about the optimal site for LUNA.14 The effectiveness of LUNA may depend on the completeness of transection of the uterosacral ligaments. Latthe found that compared to the U.K. group, the European group performed LUNA more frequently and transected the uterosacral ligament completely more often.21 The European group also transected the uterosacral ligament 2 cm or more from the point of cervical insertion more often. It is important to keep in mind the nerve plexus as described by Fujii when performing LUNA.14 It is also helpful to keep in mind that the lateral nerves will not be affected (Figure 6). The studies of Johnson and Yen indicate that LUNA does have a role to play in the relief of central pelvic pain relief not related to endometriosis.6,7 Also, the International LUNA IPD Meta- analysis Collaborative Group in 2010 found that there was no significant difference between LUNA and No LUNA for the worst pain recorded over a 12 month time period (mean difference 0.25 points in favor of No LUNA on a 0-10 point scale, 95% confidence interval: -0.08 to 0.58; P = 0.1).22 So LUNA did not result in improvements in pain, dysmenorrhea, dyspareunia, or quality of life compared with laparoscopy without pelvic denervation.23
University of Birmingham, in a randomized controlled trial in 2009 found that Among women with chronic pelvic pain, LUNA did not result in improvements in pain, dysmenorrhea, dyspareunia, or quality of life compared with laparoscopy without pelvic denervation.25
A systematic search of Duke University was performed in 2009 of the Cochrane Library and MEDLINE database for randomized controlled trials relating only to laparoscopic management of endometriosis. The information from 7 Cochrane review articles and 35 original randomized trials is presented in a clinically relevant question-and-answer format. Awareness of endometriosis as a disease with substantial morbidity is vitally important. Laparoscopic treatment of endometriosis is beneficial for reducing pain and improving fertility. Laparoscopic presacral neurectomy, but not laparoscopic uterosacral nerve ablation, is a useful adjunct to conservative surgery for endometriosis in patients with a midline component of pain. Preoperative hormonal suppression with gonadotropin-receptor hormone analogue may be helpful in decreasing endometriosis disease scores. Postoperative hormonal suppression with either a gonadotropin-receptor hormone analogue or progestin (including the levonorgestrel intrauterine system) may be helpful in reducing pain and increasing time to recurrence of symptoms.26
References
- Doyle EB. Paracervical uterine denervation by transection of the cervical plexus for the relief of dysmenorrhea. Am J Obstet Gynecol. 1955;70:11.
- Sutton C, Whitelaw N. Laparoscopic uterine nerve ablation for intractable dysmenorrhea. In: Sutton C, Diamond M, eds. Endoscopic Surgery for London: WB Saunders; 1993: 159–168.
- Lichten EM, Bombard J. Surgical treatment of primary dysmenorrhea with laparoscopic uterine nerve ablation. 1987;32:37–41.
- Gurgan T, Urman B, Aksu T, et al. Laparoscopic CO2 laser uterine nerve ablation fortreatment of drug-resistant primary dysmenorrhea. Fertil Steril. 1992;58:422.
- Sutton C. Laser uterine ablation. In: Donnez J, ed. Laser Operative Laparoscopy and Hysteroscopy. Leuven, Belgium: Nauwelaerts Printing; 1989:43–52.
- Johnson NP, Farquhar CM, Crossley S, et al. A double-blind randomized controlled trial of laparoscopic uterine nerve ablation for women with chronic pelvic pain. BJOG. 2004;111:950–959.
- Yen YK, Liu WM, Yuan CC, Ng HT. Addition of laparoscopic uterine nerve ablation to laparoscopic bipolar coagulation of uterine vessels for women with uterine myomas and dysmenorrhea. JAm Assoc Gynecol Laparosc.2001;8:573–578.
- Counseller VS, Craig W. The treatment of dysmenorrhea by resection of the presacral nerves: evaluation of end results. AmJObstet Gynecol. 1934;28:161–167.
- Owman C, Rosenbren E, Sjoberg NO. Adrenergic innervation of the human female reproductive organs: a histochemical and chemical investigation. Obstet Gynecol. 1967;30:763–773.
- Frankenhauser G. Die Bewegungenerven der Gebarmutter. ZMed Nat Wiss. 1864;1:35.
- Cleland JP. Paravertebral anesthesia in obstetrics. Surg Gynecol Obstet. 1933;57:51.
- Williams PL, Warwick R. Reproductive organs of the female. In: Williams PL, Warwick R, eds. Gray’s Anatomy. 36th ed. Edinburgh: Churchill Livingston; 1980:1423– 1431.
- Jones KD, Sutton C. Arcus Taurinus: the “mother and father” of all LUNAs. Gynecol Endosc. 2001;10:83–89.
- Fujii M, Sagae S, Sato T, et al. Investigation of the localization of nerves in the uterosacral ligament: determination of the optimal site for uterosacral nerve ablation. Gynecol Obstet Invest. 2002;54(suppl 1):11–17.
- Nezhat C, Siegler A, Nezhat F, Nezhat C, Seidman D, Luciano A. Operative Gynecologic Laparoscopy. Principles and Techniques. 2nd Edition. New York: McGraw- Hill; 2000.
- Lichten E. Three years’ experience with LUNA. Am J Gynecol. 1989;3:9.
- Davis GD. Uterine prolapse after laparoscopic uterosacral transection in nulliparous airborne trainees. A report of three cases. J Reprod Med. 1996;41:279–282.
- Good MC, Copas PR Jr, Voody MC. Uterine prolapse after laparoscopic uterosacral transection: a case report. JReprodMed. 1992;37:995–996.
- The LUNA trial collaboration, a randomized controlled trial to assess the efficacy of laparoscopic uterosacral nerve ablation (LUNA) in the treatment of chronic pelvic pain: the trial protocol (ISRCT In 41196151). Department of Obstetrics and Gynecology, Birmingham Clinical Trials Unit and Department of Public Health and Epidemiology, University of Birmingham B15 2TT, UK. BMC Womens Health. 2003;3:6.
- Latthe PM, Braunholtz DA, Hills RK, et al. Measurement and beliefs about effectiveness of laparoscopic uterosacral nerve ablation. BJOG. 2005;112:243–246.
- Latthe PM, Powell RJ, Daniels J, et al. Variation in practice of laparoscopic uterosacral nerve ablation: a European study. J Obstet Gynecol. 2004;24:547–551.
- Daniels JP, Middleton L, Xiong T, Champaneria R, Johnson NP, Lichten EM, Sutton C, Vercellini P, Gray R, Hills RK, Jones KD,Aimi G, Khan KS; as the International LUNA IPD Meta-analysis Collaborative Group. University of Birmingham, Birmingham Women’s Hospital, Edgbaston Individual patient data meta-analysis of randomized evidence to assess the effectiveness of laparoscopic uterosacral nerve ablation in chronic pelvic pain. Hum Reprod Update. 2010 Jul
- Daniels J, Gray R, Hills RK, Latthe P, Buckley L, Gupta J, Selman T, Adey E, Xiong T, Champaneria R, Lilford R, Khan KS; LUNA Trial Collaboration Laparoscopic uterosacral nerve ablation for alleviating chronic pelvic pain: a randomized controlled trial. 2009 Sep 2;302(9):955-61.
- Berkes E, Bokor A, Rigó J Jr. Treatment of endometriosis with laparoscopic surgery today. Orv Hetil. 2010 Jul11;151(28):1137-44.
- Daniels J, Gray R, Hills RK, Latthe P, Buckley L, Gupta J, Selman T, Adey E, Xiong T, Champaneria R, Lilford R, Khan KS; LUNA Trial Collaboration. Laparoscopic uterosacral nerve ablation for alleviating chronic pelvic pain: a randomized controlled trial. 2009 Sep 2;302(9):955-61.
- Yeung PP Jr, Shwayder J, Pasic RP. Laparoscopic management of endometriosis: comprehensive review of best evidence. J Minim Invasive Gynecol. 2009 May- Jun;16(3):269-81.
- Farquhar, CM, Steiner, CA. Hysterectomy rates in the United States 1990-1997. Obstet Gynecol. 2002; 99:229.
- Howard, FM. The role of laparoscopy in chronic pelvic pain: promise and pitfalls. Obstet Gynecol Surv. 1993; 48:357.
- Tu, FF, Beaumont, JL. Outpatient laparoscopy for abdominal and pelvic pain in the United States 1994 through 1996. Am J Obstet Gynecol. 2006; 194:699.
- Howard, FM. The role of laparoscopy in the chronic pelvic pain patient. Clin Obstet Gynecol. 2003; 46:749.